Lp(a) Treatment: What Works, What Doesn’t, and How to Take Control
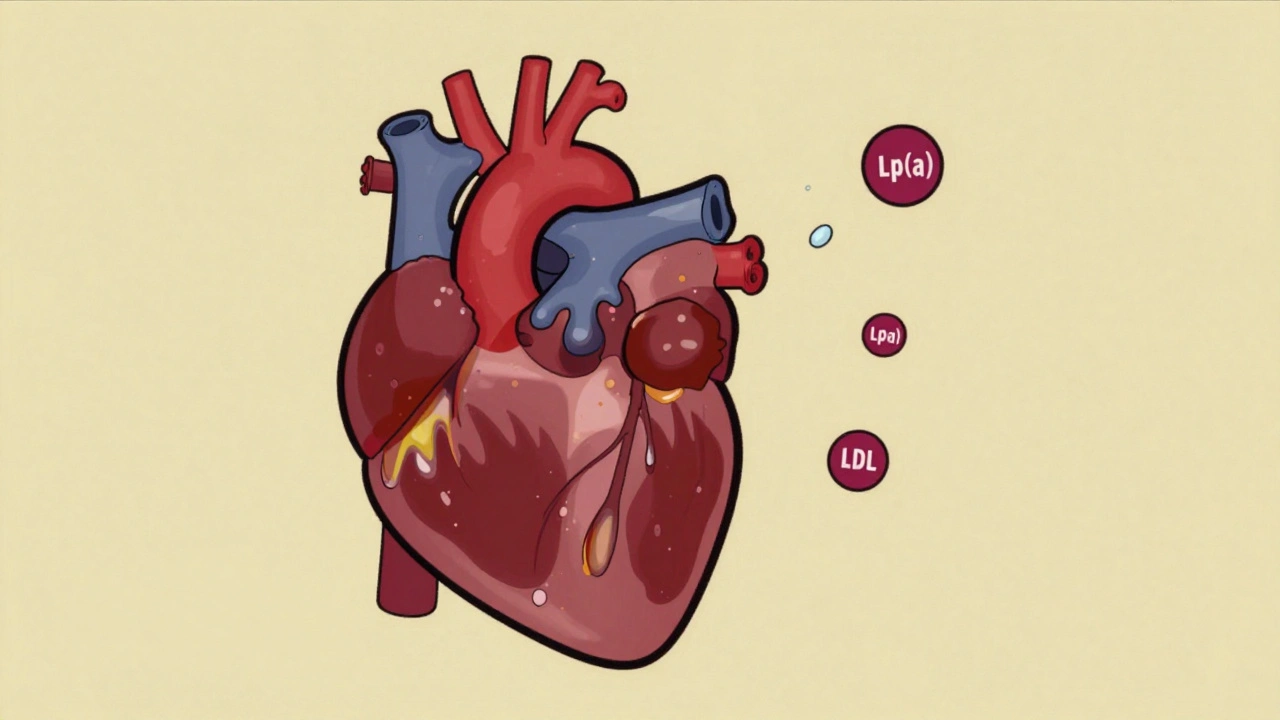
When it comes to heart disease, most people focus on LDL cholesterol—but Lp(a), a genetically driven lipoprotein that acts like LDL but sticks to artery walls and triggers inflammation. Also known as lipoprotein(a), it’s one of the most underrated risk factors for early heart attacks and strokes. Unlike regular cholesterol, Lp(a) levels are mostly set by your genes—you can’t fix them with diet or exercise alone. About 1 in 5 people have high levels, and many don’t know until they have a heart event despite eating clean and working out regularly.
That’s why lipoprotein(a), a particle that’s both cholesterol-carrying and clot-promoting is so dangerous: it slips under the radar. Standard lipid panels don’t always test for it, and even if they do, doctors often don’t know what to do next. There’s no magic pill yet, but new drugs like pelacarsen and olpasiran are in late-stage trials and show real promise in slashing Lp(a) by 80% or more. Until those are widely available, the focus shifts to managing everything else you can control—like blood pressure, smoking, and inflammation.
cardiovascular risk, the combined threat of heart attack, stroke, and vascular disease isn’t just about one number. If your Lp(a) is high, your doctor should also check your LDL, triglycerides, and C-reactive protein. High Lp(a) + high LDL is a double hit. That’s why statins are still often prescribed—not to lower Lp(a), but to reduce the rest of the damage. Some patients benefit from PCSK9 inhibitors like evolocumab, which can lower Lp(a) by 20-30%, a modest but meaningful drop. Niacin used to be used, but studies show it doesn’t improve outcomes and causes too many side effects. And don’t waste time on fish oil or plant sterols—they don’t touch Lp(a).
If you’ve had a heart attack before 55 (men) or 65 (women), or if close relatives did, ask for an Lp(a) test. It’s a simple blood draw. No fasting needed. If your level is over 50 mg/dL, you’re in the high-risk zone. That doesn’t mean you’re doomed—it means you need a smarter plan. Focus on strict blood pressure control, avoid smoking completely, and consider low-dose aspirin if your doctor says it’s right for you. Regular exercise helps your overall heart health, even if it doesn’t change Lp(a). And if you’re on a statin, make sure your LDL is below 70, maybe even 55, to offset the genetic risk.
The science is moving fast. In the next few years, we’ll likely have the first FDA-approved drugs specifically for Lp(a). But right now, your best move is awareness. Know your number. Know your family history. And don’t let a silent genetic risk slip by because no one talked about it. The posts below cover everything from how Lp(a) is measured, to real patient stories, to what new treatments are on the horizon—and how to talk to your doctor about it without getting brushed off.